Obviously, an employee or associate vet has no need to account for the bottom-line of the practice and is not interested in reducing costs. So there is no motivation to conserve resources and use just-sufficient anaesthestics as they don't bear the expenses and responsibility for the economic health of the practice. If the practice closes down, just go to another practice to work!
Just give the cat isoflurane gas by mask to continue the spay if the cat is not sufficiently anaesthesized by xylazine and ketamine. So, more isoflurane and oxygen needs to be ordered if the vet has no interest in practical research in wanting to know what is best for the cat and for the practice economics.
 Yesterday, June 6, 2012, a shy 3kg black and
white cat from Bedok came in. I used this case
to share my experience and demonstrate to Dr
Daniel how I would use an effective
optimal dosage of injectable
anaesthesia WITHOUT the need of isoflurane gas
top up. Toa Payoh Vets has the isoflurane gas
facility and so, there is no need to catherise
the cat or dog to top up, if the dosage of
injectable anaesthesia is insufficient.
However, catherisation means a waste of
resource, more time spent in
catherisation of the cephalic vein
and in topping up to get surgical anaesthesia.
This can make a spay surgery twice as long.
Yesterday, June 6, 2012, a shy 3kg black and
white cat from Bedok came in. I used this case
to share my experience and demonstrate to Dr
Daniel how I would use an effective
optimal dosage of injectable
anaesthesia WITHOUT the need of isoflurane gas
top up. Toa Payoh Vets has the isoflurane gas
facility and so, there is no need to catherise
the cat or dog to top up, if the dosage of
injectable anaesthesia is insufficient.
However, catherisation means a waste of
resource, more time spent in
catherisation of the cephalic vein
and in topping up to get surgical anaesthesia.
This can make a spay surgery twice as long.I prefer surgery to be simple and fast by giving the effective optimal dosage of xylazine and ketamine for a cat spay. I can get the whole spay done from first incision to stitching in 10-15 minutes if there is no need to top up.
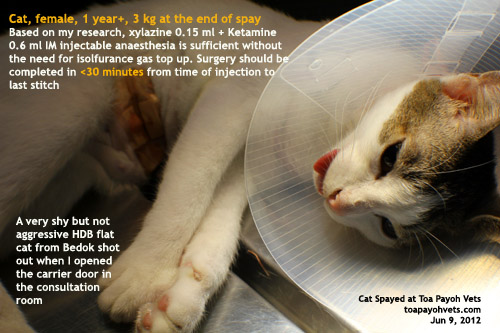
As a guideline, a cat at 3 kg needs 0.15 ml xylazine and 0.6 ml ketamine IM to be sufficiently anaesthesized without the need of isoflurane gas or top up. Dr Daniel did not think this was possible and so the isoflurane gas was switched on as standby.
However, this amount lasted more than 30 minutes and he could see that the formula was sufficient. After the IM injection of 0.15 ml xylazine and 0.6 ml ketamine, there was a wait of 10 minutes. During this time, the cat's belly was shaved.
Obviously, if the vet takes a bit longer, isoflurane gas will be needed.
TIPS
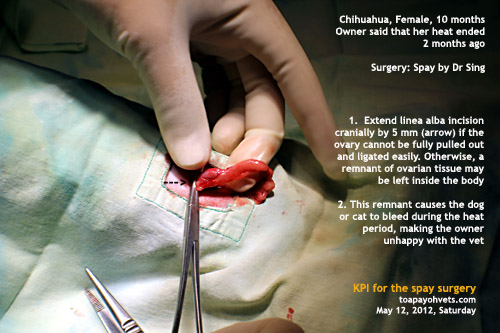
1. Don't snip off the SC fat if possible as this may lead to bleeding. Just undermine the SC fat with scissors vertically and you will see the linea alba.
2. The start of the incision is around 2 cm from the umbilical scar in a young cat.
3. This cat had enlarged congested ovaries with follicles and uterus of over 8 mm in diameter although she was never "mated". So, it was difficult to hook out the womb.
A longer incision was needed and more surgery time had to be spent. I could not believe when I saw the uterine horns being as large as 8 m min diameter and over 12 cm long. The ovarian blood vessels were enlarged and engorged. As if the cat was pregnant.
Could this be a case of cystic ovaries, pyometra or early pregnancy? However, the lady owner said: "My cat would never leave the HDB flat. Whenever she sees another cat, she would run away. It is not possible that she was mated."
"Is there a male cat in the apartment?" I asked.
"Yes, he was neutered some time ago at another vet practice."
"Did he try to mate with this caterwauling female 2 weeks ago? " I asked.
"Yes, the male cat was humping her."
So, this could be a case of false pregnancy with the signs of pregnancy in the uterus being developed. There was no foetal lumps. I did not ask Dr Daniel cut into the uterine bodies to check for foetuses. The uterus was just swollen and thicker by 100x normal for a non-pregnant young cat of around one year old. It could be a case of early pyometra.
RESTRAINT OF THE SHY CAT
As the mentor for Dr Daniel, I wanted to show how the cat would be restrained for injection. I put the cat carrier on the consultation table. A wire crate was ready. As soon as I opened the carrier door and tilted the carrier, the cat shot out like a rocket and jumped onto the floor to a corner of the back table. I expected the cat to hide inside the back of the carrier but this was not the case.
So, Dr Daniel bent on his knees and talked to the cat. He put her back into the wired crate. Now, what to do next?
"Put some telephone books inside the plastic crate to corner him and I will inject the anaesthestic," I said. But he could not find any phone books. I said: "My past practice was to put the cat inside a smaller wired crate and filled the crate with phone books so that the cat would be restrained at one corner for injection. But my staff had disposed of it during the years." So, what's the alternative?
Daniel put a large plastic carrier fit for a Jack Russell and inserted it inside the wired crate which was 30% larger. Then he put the cat inside the wired crate, attempting to corner the cat. "Ready for injection," he asked me. The cat had crawled to the top of the plastic crate and was moving. She had a long tail but that would not be useful when she was injected as she could still leap away.
"Can you inject him now?" Dr Daniel asked.
"Based on my experience, the cat will move when injected as she is not tightly cornered. Only half dose may be given."
"That should be OK," Dr Daniel replied. I knew he was thinking that there was the back up of isoflurane gas which could be used to top up the anaesthesia. But I wanted to show him in this case that an optimal injectable anaesthestic dose using xylazine 0.15 ml and ketamine 0.6 ml IM in one syringe would be sufficient. No point talking. Action speaks louder than words and this would be the case for the mentor to show the way.
"Sometimes the syringe needle may bend when the injection is given as the cat (not properly restrained) springs away," I said. In practice, it is so much different from in theory from the lectures of cat restraint. Not all cats behave the same.
"In any case, a full dose IM must be given to get the best optimal anaesthesia," I said.
As I tried to get the cat cornered, she climbed up the plastic crate top towards Dr Daniel and away from me. The cat's head peeked out from the gap of the side fence panel of the wired crate, facing Dr Daniel. He did not do anything. Neither did I.
"There is a gap in the side of wire crate which could not be closed properly after he had put in the plastic crate," Dr Daniel had not seen to this breach of security. But the cat had seen it and was now winging her way out from this gap.
It was only a gap of 8 mm but the small cat's head went out. In an instant, she sprang out and jumped onto the floor back to the corner of the floor as before.
I was quite angry at this "waste of time". The side of the wire crate was not secured properly first after the plastic crate was put in because the hooks were inside. However, this was no excuse from any vet.
The crate had a top door and Dr Daniel had dropped the cat was into the wire crate from the top while he had pushed the plastic crate through the side panel facing him. This wired crate was foldable in 6 sides and so the hooks were inside the side fence to prevent any cat escaping. That meant that, after putting inside the plastic crate, the side fence should be pushed inwards and hooked from inwards. This was not done.
So, the cat escaped again! I am not a patient mentor and I cursed. I hate wasting time which is much more precious to me at my age.
So, I left the consultation room for Dr Daniel to coax the cat back and put her into the plastic crate. Why not the wire crate? I was surprised but since now there was a new situation, I had to decide what to do, being the mentor.
"If your hand is strong enough to grip the scruff of the cat and you do not mind being scratched, hold the cat up with your hand and I will inject the back muscle" I said.
My assistant Min would hold the scruff and the back legs for the vet to inject the backside muscles. I prefer the assistant to hold the scruff of the neck with the cat held upright as that would be what the dam would do. In this case, I would know whether the assistant's grip was tight. If the cat does not move when I inject the backside muscle, that means the assistant knows what to do and has a tight grip. The cat would feel secure and motionless and there is definitely not a move when I inject the back muscle with (0.15ml xylazine + 0.6 ml ketamine in one syringe IM).
Dr Daniel did that with his left hand preparing to be clawed. He had a strong grip. The cat did not move at all when I injected. That is the norm as a strong grip on the scruff makes a cat not feeling any pain in injection, in my experience. A weak grip will result in the cat feeling the IM injection and clawing.
Then Dr Daniel put the cat inside the wire crate and from then on, he could see that a full dose IM according to my formula was really effective. He asked for isoflurane gas to be set up. I said there was no need but since he wanted it, I had the gas switched on to give him the experience as he spayed the cat. No isoflurane gas was ever needed to spay this cat. The duration of analgesia was at least 30 minutes and that was more than enough time to spay a cat.
As mentor, many optimal and safe anaesthetic lessons are taught to the younger vets by "seeing is believing"
Each young vet has his or her own ideas of anaesthesia, basically from what the vet professors have had taught them and used in the Vet School. When he comes out to work in the industry, he has to adapt to different anaesthetic and formulas which their professors had never used. This is because there is more than one combination to safely anaesthesize the cat and the vet practice has its own experienced method usually different from the Vet School which could teach and advise more injections (pre-med with ACP, sedate with another drug, atropine and other drugs) as what each professor thinks it deem fit.
One recent Melbourne Vet School graduate just recently told me that her teacher said not to use the spay hook at all. "Just make a big skin incision and use the finger to hook out the uterus," she said. So I was much surprised as the spay hook is universally used to make smaller skin incisions in a cat spay. However, each vet has his or her own way of doing surgery and some vets may find the hook not useful or effective. However, I believe that all vets doing spay should start with the spay hook first and practice makes perfect.
Surgery must be done accurately, speedily and correctly. That means using the least amount of anaesthetic safely and not to waste time in restraint and topping up with injectable or gas. I am monitoring my vets to ensure that they do a good job without wasting resources so that vet fees can be affordable. I noted that isoflurane gas is being used up more than I expected from the number of surgeries performed during my audit. "It could be the practice of using gas by mask instead of via the endotracheal tube," Dr Daniel gave me a valuable feedback. Management is to resolve problems and there seems to be one as the vets could be giving below optimal dosage for spays, leading to a need to top up with isoflurane gas.