|
Toa Payoh
Vets Clinical Research
Making veterinary surgery alive
to a veterinary student studying in Australia
using real case studies and pictures |
Know both the fundamentals and technicals to succeed in
veterinary medicine - vomiting in a dog
Dr Sing Kong Yuen, BVMS (Glasgow), MRCVS
Date:
11 April, 2010 |
 toapayohvets.com toapayohvets.com
Be Kind To Pets
Veterinary Education
Project 2010-0129 |
April 7, 2010.
Perth, 6 am. Writing from a Willeton house in
Perth as I reflected on this "medical malpractice"
case.
Vet 1 diagnosed kidney failure.
The adult neutered male dog of a small breed,
around 5 years had been vomiting for the past few
days and occasionally over the years. Vet 1's
blood test some 9 months ago showed a high BUN. So
she advised another blood test. It showed high BUN
and an extremely high creatine level. She
suspected acute kidney failure and advised
abdominal scanning at two other practices as she
does not have the facility. Antibiotics were
prescribed for the "skin disease" according to the
owner.
Vet 2 (myself) advised monitoring.
The worried owner phoned me wanting to
fax me the blood tests and get a telephone
diagnosis. I asked her to bring the dog down for
an examination as blood test results need to be
co-related with the history and physical
examination of the dog.
She got the dog in for examination. She showed me
the blood tests and asked whether her dog was
dying soon. The dog was normal and had no
polydipsia or polyuria. Therefore, I did not "run
down" the other vet. I did not ask for another
blood test to verify as it was taken 24 hours ago.
I presumed that the owner would not want one as
most owners of small breeds feel the pain of their
dogs having their small vein punctured for blood
taking. In any case, most vets in Singapore,
including me, trusted the blood test results of
our competitors and seldom asked for another test.
This was a big mistake on my part.
As the dog was active and normal, except for
vomiting, I said it was not dying soon. It could
be having gastritis (stomach infection). I advised
taking of the antibiotics I prescribed for 5 days.
The important thing was to monitoring the water
intake daily and to keep in touch by phone if
vomiting persisted and the dog did not eat. I
advised a prescription canned food for kidney
disease. The owner phoned me the next day that the
dog ate the canned food. However, it vomited after
eating the canned food some 24 hours later.
Vet 3 diagnosed no kidney problems. The
owner went to Vet 3 to get a scan. Vet 3 did a
blood test and warded the dog which was given an
IV drip. "It is a medical malpractice," the owner
phoned me. "Vet 1 said that her blood test machine
had broken down and did not even have the decency
to phone me earlier." There was much anger. There
was a meeting with Vet 1. Vet 1's mentor told the
owner that I ought to have taken a blood test.
Since I had not done it, I was also involved in
"misdiagnosis".
Conclusion:
I should have taken a blood test and recommended a
scan immediately. There was no point trying to
save money for the owner. Practising defensive
medicine would have been prudent on hindsight. I
apologised for not having asked her to take a
blood test. She said she would have objected
anyway. I offered to take back the cans
prescription renal diet.
"Well, Vet 3 says that the dog should be on a
prescription liver diet!". The dog was no more
vomiting. What was the diagnosis? Liver problems
now? This case shows that the vet must get another
blood test done and if the owner objects, to put
it in writing. If the physical findings do not
indicate kidney failure, be assertive and run down
the competitor. No quarters given. However,
running down the competitor just adversely affect
the image of the veterinary profession in
Singapore. I don't do it. Every vet will make
mistakes and so I don't run down my competitors. I
hope the 4th year vet students in Murdoch
University will find this case alive and
interesting for their "Polydipsia and Polyuria"
lectures, well documented by Dr Peter Irwin,
1. Normal dogs drink about 50-60 ml/kg/day. Cats
considerably less. I did ask the owner to monitor
the water intake. Instead she syringe feed water
to the dog. This may be one cause of "vomiting"
after eating the canned food.
2. Polydipsia: >100ml/kg/day in dogs. >50ml/kg/day
in cats on DRY food and >10ml/kg/day in cats on
WET food.
3. Polyuria: increase in urine production
>50ml/kg/day. general guide only. not possible to
measure in clinic or home setting.
4. Urine Specific Gravity (USG) to assess
renal concentrating ability. Measured on a
refractometer (urine dipstick results unreliable).
No such thing as a "normal" USG. Most healthy
animals USG 1.025 to 1.065. A sample with <1.025
may raise a diagnostic suspicion of polydipsia.
4.1 Hypersthenuria USG>1.012. Urine more
concentrated than the patient's plasma
4.2 Isothenuria USG 1.008 - 1.012. Persistent
isothenuria with azotaemia is consistent with
tubular insufficiency or renal failure.
4.3 Hyposthenuria USG <1.008. Renal tubules can
dilute but not concentrate urine. Unlikely to have
renal failure or insufficiency. Usually caused by
interference with the ADH receptors in the renal
collecting ducts.
DDx of PU and PD in dogs and cats
COMMON CAUSES
DOGS
Chronic renal disease
pyometra
diabetes mellitus
hyperadrenocorticism
Iatrogenic (drug induced)
Medullary solute washout - a process as a
consequence of marked polyuria of ANY CAUSE and
can contribute to the severrity of the PU. E.g.
relief of Urinary tract obstruction in FLUTD cat.
CATS
Chronic renal disease
Post-obstructive diuresis
Hyperthyroidism
Diabetes melllitus
Iatrogenic
Medullary solute washout
P.S. It is best to advocate ultra-scan of
the kidneys to check for polycystic kidneys or
tumours and not to ask the owner to wait a few
days. In the above case, the owner said that Vet 1
should have made the necessary arrangements as she
was told to wait 2 weeks at one practice. She
managed to find one vet who did the scan.
LESSONS LEARNT FROM THIS CASE
1. PROVIDING EXCELLENT CUSTOMER SERVICES
The vet can make arrangements for scanning at
other practices since he has none. The dog owner
wants scanning and therefore, this service should
create goodwill and loyalty if the vet does it. As
for me, I did not advise immediate scanning as my
clinical findings did not indicate acute renal
failure and like vets from my baby-boomer
generation, I was trying to lower the owner's
total veterinary costs. I should make arrangements
for scanning as that was what the owner wanted. In
fact, she had the impression that I said scanning
was unnecessary, according to Vet 1's mentor when
I spoke to him to discuss the resoluion of the
owner's conflicts in this case.
2. MINI-PROFILES NOT ADVISED
Always collect URINE and blood for health
screening. This is because the vet cannot assess
the dog's metabolic state without both samples. In
this case, Vet 1 did a mini-profile to check only
blood BUN and creatinine. The owner told me that
the BUN was high but creatinine was normal some 9
months ago and the vet advised a mini-profile to
check BUN and creatinine. The BUN has gone higher
and the creatinine level was extremely high in the
second mini-profile test.
FULL PROFILE means CBC (complete blood
count) and FBE (full biochemical exam) AND
elecrolytes (Na, Cl & K). Many Singapore
pet owners will not want to pay for the full
profile and so, permission must be given first.
Otherwise, the owner may not pay!
3. HONESTY
The owner complained that Vet 1 should have had
informed her when the vet knew that the blood test
machine was malfunctioning instead of after she
told them that Vet 3 had said that there was no
kidney disorders from Vet 3's blood test. She had
to take leave from work and suffered stresses.
"Why didn't Vet 1 inform me earlier?" she said.
"It is medical malpractice!"
4. REPEAT BLOOD SAMPLE.
I should have strongly advise a blood
sample plus a urine sample when clinical
findings did not indicate an acute renal failure.
This was what the owner had the impression from
Vet 1 and was worrying a lot. I was trying to save
the owner some money. Younger vets in Singapore do
not think twice about blood tests, X-rays, urine
tests and histopathology (even for a hamster
tumour). Times have changed and the Singapore pet
owner must pay more for vet treatment.
5. POLYDIPSIA AND POLYURIA
Many Singapore dog owners know that their dogs
drink a lot but don't know how much. The dog may
not be polydipsic. Check Urine SG with a
refractometer. A sample with less than
1.025 may indicate polydipsia.
6. ACUTE RENAL FAILURE
is characterised by the sudden onset of oliguria/anuria,
azotaemia or both.
6.1 Clinical Signs are: extreme lethargy (the dog
was active in this case study), dehydration,
oliguria or anuria and vomiting.
6.2 Lab findings include: renal azotaemia (very
high increase in BUN and creatinine) with
isothenuria. Urea >50mmol/L. creatinine
>300mmol/L.
6.2.1 Urine analysis may show cause e.g. oxalate
crystals, white cell cass, bacteriuria in acute
pyelonephritis).
6.3 Electrolyte abnormalities (Na, K, Cl variable)
6.4 Metabolic acidosis
6.5 Hyperphospataemia
I hope this case study will be useful as they show
the owner's points of view. In this case, assuming
that the blood test machine was not
"malfunctioning", it is possible that the vomiting
dog had a bacterial infection of the kidneys
resulting in a renal azotaemia (acute renal falure).
With antibiotics, the dog took a few days to
recover. When Vet 3 was consulted, there was no
more bacterial infections (e.g. pyelonephritis)
and therefore no more renal azotaemia. Acute renal
failure at the beginning stage may just show
azotaemia and not oliguria/anuria. So Vet 3 became
the hero. A urine test by Vet 1 would have been
very useful to support bacterial infection in the
urinary tract, e.g. proteinuria, white cell casts,
USG, pH, presence of uroliths but the owner might
not want to pay initially and this is a common
situation in Singapore in this period of
recession.
CONCLUSION
4th year vet students who must study a lot of
theories and memorise them to pass examinations
can see that the complexities and and economics of
practice are so much different from the class-room
lectures.
Mini-profile blood tests rather than complete
blood count and biochemistry may be done in
practice as the owner may not want to pay for a
comprehensive blood test. Do NOT assume
that the owner would not want a repeat blood test.
Get a second blood test done rather than try to
save money for the owner and be liable for
"medical malpractice" litigation. Get the owner's
objection recorded if the owner does not want a
second blood test.
|
|
|
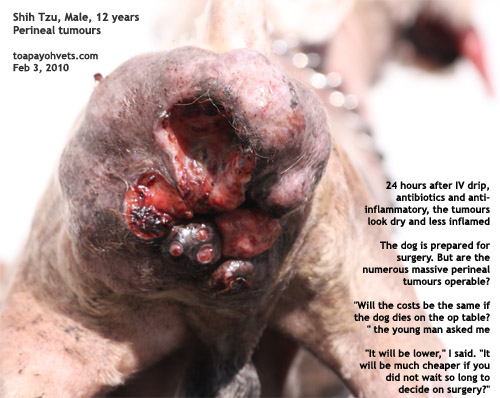
 BE
KIND TO OLDER DOGS & CATS ---
GET TUMOURS REMOVED EARLY ---
WHEN THEY ARE SMALLER BE
KIND TO OLDER DOGS & CATS ---
GET TUMOURS REMOVED EARLY ---
WHEN THEY ARE SMALLER
More case studies, goto:
Cats or
Dogs |
|
|
To make
an appointment: e-mail
judy@toapayohvets.com
tel: +65 9668-6469, 6254-3326 |
toapayohvets.com
Be Kind To Pets
Veterinary Education
Project 2010-0129 |
|
|
 Toa
Payoh Vets Toa
Payoh Vets
Clinical Research
|
|
|
Copyright ©
Asiahomes Internet
All rights reserved. Revised: April 11, 2010
Toa Payoh Vets
|
|